Diphtheria Factsheet for Health Workers
Overview
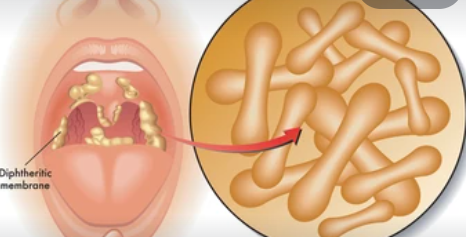
Diphtheria is a vaccine-preventable disease caused by bacteria of the Corynebacterium species. It is mostly caused by toxin-producing Corynebacterium diphtheriae and rarely by toxin-producing strains of C. ulcerans and C.pseudotuberculosis.
The most common type of diphtheria is classic respiratory diphtheria, whereby the exotoxin produced characteristically causes the formation of a pseudo-membrane in the upper respiratory tract and damages other organs, usually the myocardium and peripheral nerves. Acute respiratory obstruction, acute systemic toxicity, myocarditis, and neurologic complications are the usual causes of death.
In the 2022 diphtheria outbreak in Nigeria, common causes of death include respiratory distress, Acute kidney injury (AKI), heart disease (Myocarditis), and Bleeding disorders. Infection can also affect the skin (cutaneous diphtheria). More rarely, it can affect mucous membranes at other non-respiratory sites, such as genitalia and conjunctiva.
Currently, there is an outbreak of diphtheria in Lagos State and the Emergency Operations Centre has been activated to control and prevent further spread of the disease.
Transmission
C. diphtheriae is transmitted from person to person by close and direct contact (respiratory secretions) when an infected individual coughs or sneezes, in contrast, C. ulcerans and C. pseudotuberculosis are zoonotic infections, not transmitted from person to person.
The incubation period of C. diphtheriae is two to five days (range 1– 10 days). A person is infectious when virulent bacteria are present in the respiratory secretions, usually two weeks without antibiotics, and seldom more than six weeks. In rare cases, chronic carriers may shed organisms and transmit the infection for six months or more. Skin lesions are often chronic and infectious for longer periods. Effective antibiotic therapy promptly terminates shedding in about one or two days.
Clinical Presentation
Symptoms often appear 2 to 5 days post-exposure and may include:
- Sore throat
- Fever
- Malaise
- Swelling of the neck (bull neck appearance)
- Difficulty swallowing
- Hoarseness
- A characteristic grayish white pseudomembrane in the throat
Severe Complications:
- Myocarditis (inflammation of the heart muscle)
- Peripheral neuropathy (nerve damage)
- Airway obstruction, which can lead to respiratory failure and death if untreated.
Diagnosis
- Clinical Diagnosis: Identified by symptoms, especially the characteristic pseudomembrane in the throat.
- Laboratory Diagnosis:
- Throat cultures isolate diphtheriae.
- PCR (Polymerase Chain Reaction) testing to detect bacterial DNA.
- Elek test to confirm toxin-producing strains of diphtheriae.
Case definitions
Standard Case definition
• A suspected case of diphtheria is defined as a case of an upper respiratory tract infection characterized by:
• laryngitis or pharyngitis or tonsillitis.
AND
• adherent membranes of the tonsils, pharynx, and nose
Diphtheria Case is said to be a confirmed case if it meets the following criteria:
• A Laboratory-confirmed case of diphtheria is defined as a person who has Corynebacterium spp. isolated by culture and is positive for toxin production, regardless of symptoms.
Clinical management
Management of diphtheria is a multi-disciplinary care involving various specialties such as, pediatrician, Infectious disease specialist, ENT specialist, cardiologist, pulmonologist, nephrologist, neurologist, hematologist, dietician, intensivist, nurses etc. Ideally all suspected cases should be managed in a dedicated isolation unit or centre which should comprise of a triage, inpatient ward, contacts clinic, follow up and immunization unit.
Definitive therapy
Neutralization of circulating toxins:
DAT [Diphtheria AntiToxin] is the mainstay of treatment and should be administered (ideally within 1 hour of dmission) as soon as possible in a hospital setting. Disease course and outcome depends on how early antitoxin treatment is started; after about three days from onset, the risk of complications and fatal outcome increases with each passing day if DAT administration is delayed.
DAT is administered only once following sensitivity screening. If diphtheria is strongly suspected, treatment with DAT should be given immediately without waiting for laboratory results, preferably intravenously in serious cases and intramuscularly otherwise (see appendix on the modalities of IMadministration). The dose of DAT varies depending on site and extent of pseudo membrane, time of onset and severity of infection.
The protocol for DAT administration is attached to this factsheet.
Diphtheria Antibiotic Management
- Oral Azithromycin 10-12mg/kg [maximum of 500mg/day] for 14 days
- Oral Erythromycin All persons: 40 mg/kg/day (maximum, 2 gm/day) dose,
10 mg/kg every 6 hours, maximum 500 mg per dose.
Treat for total 14 days.
Do not give < 2 months of age.
Detail management is contained in the attached National Guidelines for Diphtheria
Response.
Infection Control Measures
- Isolation: Isolate suspected or confirmed cases to prevent the spread of the disease.
- Personal Protective Equipment (PPE): Health workers should use masks, gloves, and other PPE while caring for infected patients.
- Standard and Droplet Precautions: Employ these precautions to minimize the risk of transmission.
- Surface Cleaning: Ensure thorough cleaning and disinfection of surfaces and equipment that may be contaminated.
Reporting and Surveillance
Any suspected case should be reported to the LGA Disease Surveillance and Notification Officers [DSNO] for further investigation. Report can also be sent to the State Epidemiologist or the State DSNO by calling the following GSM numbers 08023169485 0r 08137412348


{kind=link}